
Binocular Vision – Easier Than You Think (Lecture)
This one hour lecture, delivered to final year QUT optometry students, describes a simplified two-system approach to BV diagnosis and management.
This one hour lecture, delivered to final year QUT optometry students, describes a simplified two-system approach to BV diagnosis and management.
From a myopia control point of view, esophoria and accommodative lag are the key clinical red flags in assessing your patient’s visual efficiency, and thankfully both will usually respond positively to a near addition.

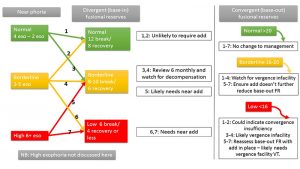
Kate describes near heterophoria to her patients as where their eyes aim in space – the posture of their vergence system – and esophoria is our key enemy in the myopia control battle.

Assessing horizontal fusional reserves at near gives you the measure of your patient’s stamina, or ‘petrol in the tank’ to be able to manage their phoria, or ‘posture’.

What causes myopic progression? Studies have attempted to find causative factors related to genetic, environmental, and behavioral influences including parental myopia, time spent outdoors, and hours of near work (reading, computer, video games).1

Center-distance soft multifocal contact lenses have been shown to slow the progression of myopia,1-5 but practitioners around the world are concerned about the vision produced by soft multifocal contact lens wear in children.
For you and I, as eyecare practitioners, it means to balance the needs of our patients, our work, our families, and our work/life balance in harmony.
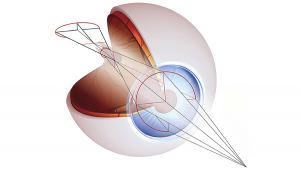
This experimental design was primarily based on the peripheral retinal blur theory, that E. Smith developed,1 providing an incremental, progressive, refractive change from the central visual axis to peripheral retina, reaching a +2.00D add plus power at about 35 degrees of retinal eccentricity and achieving about +6.00D of addition plus power at the edge of the optical zone (4mm semichord diameter).

In this short video, I introduce Myopia Profile, explain how I use it in practice, and describe two typical childhood myopia cases.
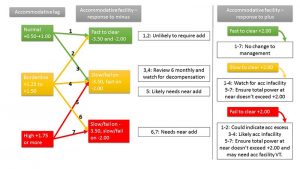
Given that a normal lag result is +0.50, I would generally prescribe an add which is the accommodative lag result subtracting 0.50, so the resulting final lag is within the normal range. For example, a lag of +2.00 results in a +1.50 Add; a lag of +1.50 results in a +1.00 Add. However, this formula may not work if:


